
West Bengal Solved Healthcare Access. It Hasn't Solved Health.
Institutional deliveries are near-universal. Maternal mortality hasn't improved. The data explores why.

This is Part 3 of the West Bengal Data Series. Part 1 looked at Kolkata versus India’s other megacities. Part 2 examined West Bengal’s investment and industrial structure.
If this series has been useful, subscribe below.
India is the world’s fourth (or fifth) largest economy by nominal GDP. By per capita income, it ranks 136th. That gap is the context for everything that follows here.
At that income level, the ability of most citizens to purchase private healthcare is alarmingly limited. The quality of the public system is not a policy preference. It is essential for survival & wellbeing, which means that when you want to understand how a state is doing, the health numbers are among the most honest data available. They reflect what the system actually delivers to people who cannot opt out of it.
This piece looks at West Bengal’s health profile across five indicators: infant mortality, maternal mortality, anaemia, institutional delivery coverage, and public health financing. Some numbers are good. Others are not. Together, they describe a state that has solved one set of problems and left another untouched.
The IMR picture
West Bengal’s infant mortality rate is 17 deaths per 1,000 live births. That places it alongside Karnataka, well ahead of states like MP, UP, Gujarat, and comfortably below the national average of 25. The improvement over the past decade has been steady and real.
Infant mortality rate measures deaths in the first year of life per 1,000 live births. It is one of the most widely used proxies for a state’s health system because it captures nutrition, maternal care, immunisation coverage, and access to neonatal facilities in a single number. A state that does well on IMR has typically gotten several things right simultaneously. That is quite important for an Indian state.
Across nearly a decade, West Bengal has consistently outperformed India on this measure. The gap has been consistent.
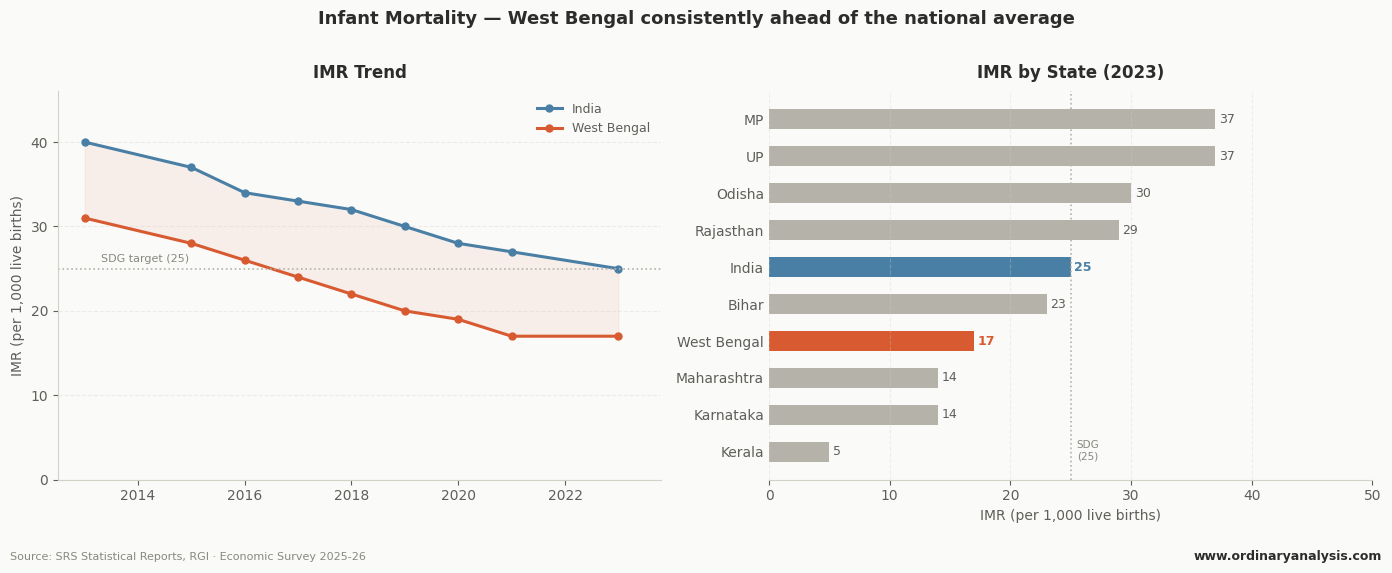
The improvement from 31 in 2013 to 17 in 2023 tracks better than the national pace. On under-five mortality1, West Bengal has already met the 2030 SDG target of under 25. Bihar and Uttar Pradesh are still in the 30s.
The MMR reversal
Maternal mortality tells a different story. A sharply different one.
In 2014-16, West Bengal’s MMR was 101 deaths per 1,00,000 live births. India’s was 130. West Bengal was not just better than average. It was well ahead.
Then something shifted.
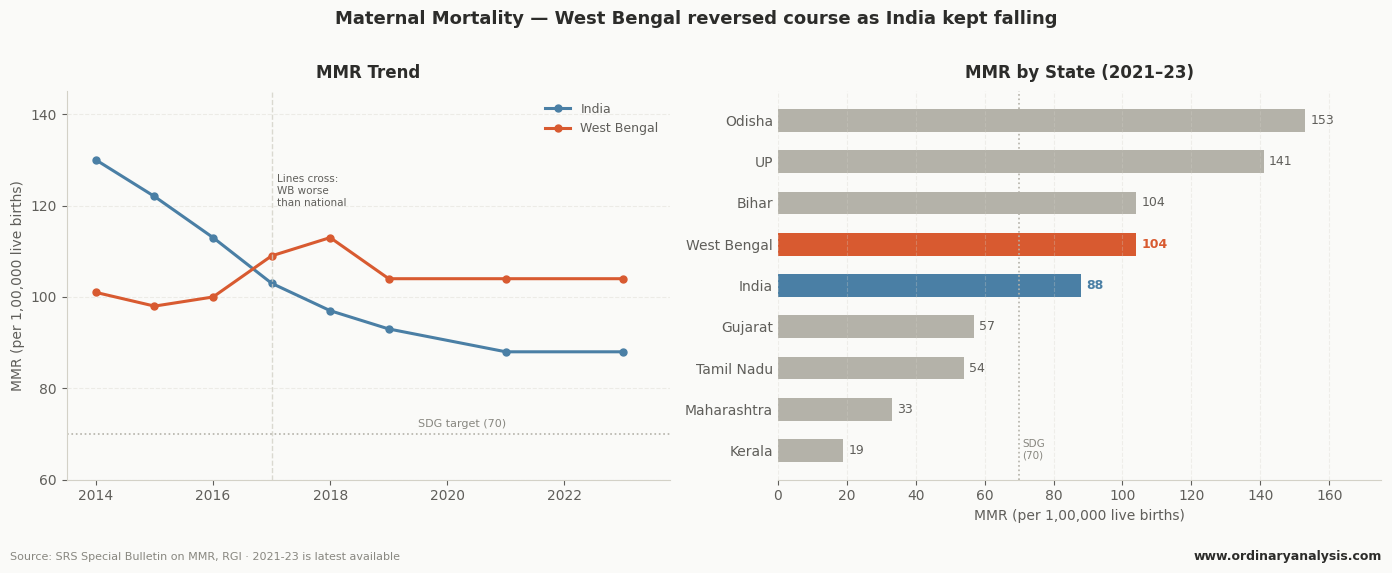
India kept improving. West Bengal did not. By 2017-19, the lines had crossed. India’s MMR fell to 103. West Bengal’s had climbed to 109. By the latest available data, India sits at 88. West Bengal is at 104, grouped with Bihar, well above states like Tamil Nadu (54), Maharashtra (33), and Kerala (19).
West Bengal is one of only four states where MMR increased against the national declining trend between survey periods, alongside Haryana, Uttarakhand, and Chhattisgarh2. A peer-reviewed study in Scientific Reports found that while most major states showed a broadly linear decline in MMR from 2014 to 2020, West Bengal showed a cyclical pattern, stagnating where others improved.
The infant survives. The mother does not, at rates that have stagnated over the last few years.
The access explanation does not hold
Poor MMR often stems from poor access to better institutional care. Women delivering at home, without skilled attendance, without emergency obstetric backup. It follows the basic logic.
That explanation does not fit West Bengal’s numbers3.
Institutional deliveries rose from 75.2% in NFHS-4 to 91.7% in NFHS-5. Nine in ten births now happen in a medical facility. Crucially, the cost of delivery in public facilities actually fell over this period, by Rs 5,236 per delivery on average. The access problem, to the extent it existed, has been substantially addressed.
West Bengal got more women into hospitals. But the MMR didn’t improve.
This points to a quality problem, not an access problem. Women are reaching facilities. What happens inside those facilities, and the condition women arrive in, is the unresolved question.
The anaemia evidence
The condition women arrive in is measurable and may be a more important causal factor of why the MMR numbers have stagnated. Anaemia prevalence is one of the strongest predictors of maternal mortality risk. It reduces the body’s capacity to manage blood loss during delivery, increases the risk of preterm birth, and amplifies every other complication.
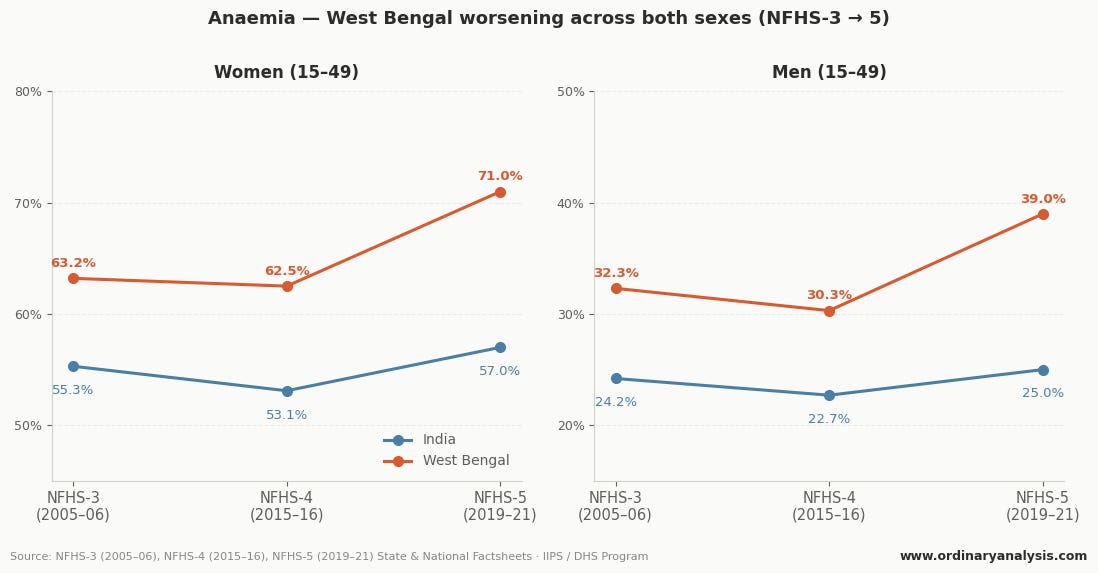
West Bengal’s anaemia numbers are not just high. They are worsening, and they have been worsening across three survey rounds.
Among women aged 15-49, prevalence increased from 63.2% in NFHS-3 (2005-06) to 62.5% in NFHS-4 (2015-16), and then jumped sharply to 71% in NFHS-5 (2019-21). India’s national average is 57%. West Bengal has the highest prevalence of anaemia among women of any large state in the country.
This is not a story of a state that made progress and then slipped. Anaemia among women was high in 2005, remained high through 2015, and then deteriorated further. The NFHS-4 to NFHS-5 spike of nine percentage points is one of the largest increases recorded among major states in the period.
The men’s numbers add context. Anaemia among men aged 15-49 dropped marginally from NFHS-3 to NFHS-4, from 32.3% to 30.3%, then rose sharply to 39% in NFHS-5. India’s national average is 25%. This is not solely a women’s nutrition story. It is a systemic public health condition that affects the state’s population broadly.
What the budget says
A state with anaemia at 71% among women is a state with a chronic nutritional deficit that predates healthcare delivery. Reversing it requires sustained investment in public health infrastructure, nutrition programmes, and preventive care.
West Bengal allocated 6.4% of its total expenditure to health in 2025-26, marginally above the national state average of 6.2%. On that metric, it appears to be doing its share.
The more telling number is out-of-pocket expenditure. Per capita OOPE in West Bengal is Rs 4,010 annually4, the second highest in the country after Kerala. Over 50% of total health expenditure in the state comes directly from household spending, not government funding.
Kerala’s high OOPE reflects a wealthy population choosing premium private healthcare on top of a functional public system. West Bengal’s high OOPE reflects a public system that is not absorbing enough of the healthcare burden. Patients are paying because the alternative is inadequate.
The 2026-27 interim budget, tabled ahead of the state elections, allocated 7.5% of GSDP to social services spending. Capital outlay, the spending that builds infrastructure, has consistently undershot budget estimates by 20-34% in recent years. What is budgeted and what is built are different numbers.
The summary
West Bengal is a state that has successfully reduced infant mortality to near-southern-state levels. That is a genuine achievement, and the data is clear on it.
The same data shows a maternal mortality rate that stopped improving a decade ago and has since worsened relative to the national average. It shows anaemia among women at 71%, the highest of any large state, rising across three survey rounds. And it shows a public health financing structure where households bear more than half the cost of care.
West Bengal did the work on access. Institutional deliveries are near 92%. The gap is not in whether women reach hospitals. It is in the condition they arrive in, and in whether the infrastructure they reach is equipped to manage it.
The next piece in this series looks at literacy, education, and human development.
Observations, data, and the not-so-ordinary world. Subscribe if that's your kind of thing.
Share it with someone who you think would enjoy it.
Data Source:
SRS Special Bulletin on MMR (RGI),
SRS Statistical Reports
NFHS-3/4/5 State Factsheets (IIPS/DHS Program)
PRS Legislative Research Budget Analysis 2024-25 and 2025-26
National Health Accounts 2021-22 (MoHFW)
Contributing factors for reduction in maternal mortality ratio in India: https://www.nature.com/articles/s41598-024-65009-0
West Bengal's Under-Five Mortality Rate (U5MR: deaths before age 5 per 1,000 live births) stood at 20 in 2021, already below the 2030 SDG target of 25. IMR and U5MR are related but distinct. The U5MR number is always higher as it includes infant deaths plus deaths between the ages of 1 and 5.
I honestly don’t know how to make sense of this. How is the IMR improving, and the MMR is not?
This is not only a West Bengal thing. A simple linear regression of institutional delivery rates against MMR across 16 major states (NFHS-5 / SRS 2019-21) shows a negative slope, as expected, but a weak fit: R² = 0.13, p = 0.16. Institutional delivery rate explains roughly 13% of the variance in MMR across states. The relationship is directionally correct but statistically insignificant. This is not a West Bengal-specific finding. It holds for the full set of states. Access to institutional care is a necessary condition for reducing maternal mortality, but not a sufficient one. West Bengal sits 24.5 MMR points above what its institutional delivery rate would predict, making it the clearest illustration of a broader pattern: moving women to hospitals without addressing the conditions they arrive in, like nutrition, anaemia, and care quality, leaves the harder problem unsolved. If we could have gotten patient-level data for this, then that would have been quite helpful.
WB's per capita income is below the national average. The argument that high OOPE reflects consumer preference for private care is stronger in richer states. In WB, it more likely reflects public system gaps.